Tetanus
A bacterium called Clostridium tetani is responsible for tetanus is. It is found in vegetative form or, in unfavourable environmental situations, in the form of spores.
The vegetative form usually lives in the intestines of animals and is scarcely resistant in the external environment. The spores, on the contrary, are highly resistant and, expelled through faeces, can persist for years in the environment. In the vegetative phase the microorganism produces a toxin responsible for clinical cases of the disease.
Transmission routes
Tetanus can come from trivial or inapparent wounds contaminated by tetanus spores. It is not transmitted from person to person. If the ideal conditions persist, ie lesions with no oxygen present, the spores germinate giving rise to vegetative forms and the consequent production of the toxin.
Symptoms and complications
Once it enters the body through a wound, the tetanus toxin is able to reach the central nervous system through the bloodstream or the nerves. Once present in the central nervous system it compromises the transmission of inhibitory impulses at the level of the synapses, causing widespread contractions and spasms. The incubation period varies from 3 to 21 days, and usually lasts for around 8 days. In general, the further the site of the wound is from the central nervous system, the longer the incubation period. Various forms of tetanus have been described:
- local tetanus: this is rare, and is characterised by persistent muscle contractions in the area of the wound. These contractions can persist for many weeks before they gradually disappear. Only 1% of cases are fatal.
- cerebral tetanus: this is rare and presents with otitis media (ear infections) in which C. tetani is present in the middle ear flora, or following head injuries.
- generalised tetanus: this is the most common type (about 80%). The disease usually presents with symptoms which reduce over time. The first sign is trismus or the contraction of the masseter muscle, giving the patient's face a characteristic appearance (lockjaw), followed by stiffness of the neck, difficulty swallowing, and stiffness of the abdominal muscles. Other symptoms include high temperature, sweating, high blood pressure, tachycardia. Spasms can occur frequently and last for several minutes. The patient remains conscious and muscle spasms, caused by even minimal stimuli, cause pain. Spasms continue for 3-4 weeks. Complete recovery can take months.
- neonatal tetanus: this is a form of generalised tetanus that occurs in newborns. It affects children born to unvaccinated mothers; they therefore do not have the protection usually given in the first months of life by maternal antibodies. It usually occurs through infections of the unhealed umbilical stump, in particular when the cord is cut with a non-sterile instrument. The symptoms are those of generalised tetanus, with a high mortality rate. Neonatal tetanus is common in some developing countries and caused more than 257,000 deaths per year worldwide over the period 2000-2003.
Tetanus can cause several complications. Spasm of the vocal cords and/or of the respiratory muscles such as to impair breathing leads to respiratory problems. Muscle spasms can cause fractures of the spine or long bones. Hyperactivity of the autonomic nervous system can lead to hypertension or arrhythmia. In recent years, tetanus has been fatal in about 11% of reported cases. The cases that are most likely to be fatal are those occurring in people over 60 (18%) and unvaccinated individuals (22%).
The fatality rate of tetanus is about 50%.
Impatto sulla popolazione
WHO reports a reduction in tetanus cases worldwide related in part to the increase in vaccination coverage, and in 2011 reported 14,132 cases of tetanus throughout the world. From 2008 to 2010 there were an estimated 61,000 deaths caused by tetanus.
Table 1 shows the data relating to the cases of tetanus reported in Italy from 1971 to 2000. There has clearly been a sharp reduction in the number of cases detected in the country dating from the introduction of compulsory vaccination in children in the early 1960s.
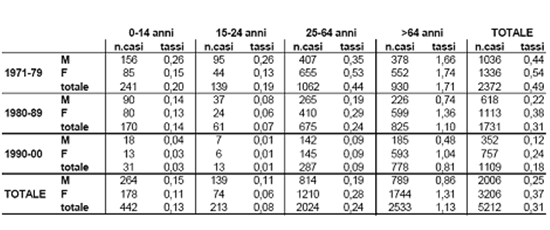
Table 1: Tetanus cases and incidence rates reported in Italy from 1971 to 2000, by gender and age group (source: Epicenter)
Subsequently, as shown in Graph 1, the decrease in cases has followed a more gradual trend. The lowest ever incidence was reached in 2005 with 49 cases (Table 2); in 2010, 58 cases of tetanus were reported to the ECDC (European Centre for Disease Prevention and Control).
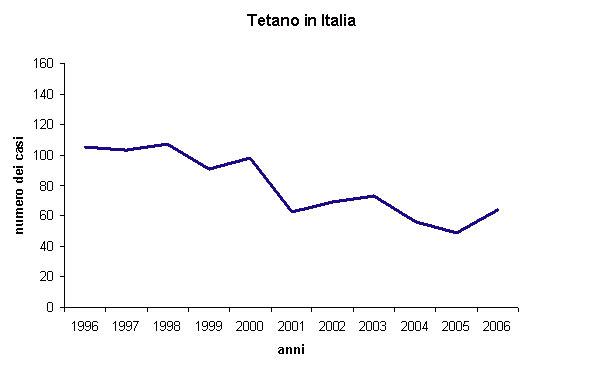
Graph 1: Number of tetanus cases reported annually in Italy from 1996 to 2006 (source: Epicenter).
| Anno | M | F | Totale |
|---|---|---|---|
| 1996 | 31 | 74 | 105 |
| 1997 | 31 | 72 | 103 |
| 1998 | 38 | 69 | 107 |
| 1999 | 25 | 66 | 91 |
| 2000 | 34 | 64 | 98 |
| 2001 | 19 | 44 | 63 |
| 2002 | 22 | 47 | 69 |
| 2003 | 18 | 55 | 73 |
| 2004 | 16 | 40 | 56 |
| 2005 | 10 | 39 | 49 |
| 2006 | 26 | 38 | 64 |
Table 2. Number of tetanus cases in Italy from 1996 to 2006 (source: Ministry of Health)
All cases of tetanus observed in Italy over the past few years concern people who had never been vaccinated, or were not adequately vaccinated (<3 doses, or intervals of over 10 years from the last dose). In most cases of tetanus reported in recent years, the infection was caused by minor injuries or excoriations.
Sources / Bibliography
- Manuale Merck online
- ECDC Surveillance – Relazione epidemiologica annuale 2011
- Dati Epicentro
- Dati WHO 2011
- Piano Nazionale Prevenzione Vaccini 2012-2014
- Epidemiology and Prevention of Vaccine-Preventable Diseases, The Pink Book: Course Textbook, 12th Edition Second Printing (May 2012)
